PHYSICAL THERAPY GUIDE TO BED SORES

A PRESSURE ULCER, SOMETIMES CALLED A “BED SORE,” IS A SKIN INJURY THAT OCCURS IN ABOUT 40,000 PEOPLE EVERY YEAR. USUALLY, PRESSURE SORES HAPPEN WHEN PEOPLE ARE VERY ILL FOR A LONG PERIOD OF TIME AND ARE NOT ABLE TO CHANGE THEIR POSITION IN A BED OR A CHAIR. PEOPLE WHO HAVE CONDITIONS SUCH AS DEMENTIA AND SPEND A LOT OF TIME IN A BED OR A CHAIR MIGHT NOT EVEN REALIZE THAT THEY NEED TO CHANGE THEIR POSITION.
What Is a Pressure Ulcer |Bed Sore?
PRESSURE ULCERS ARE CAUSED BY FORCES THAT BLOCK THE FLOW OF BLOOD TO THE SKIN:
- When too much pressure being exerted on the same area of the skin for too long, such as when someone lies in the same position all the time.
- When “shearing” forces cause the skin to bunch up in one area, such as when a person stays in a reclining position too long in either a bed or a chair.
PRESSURE ULCERS CAN HAPPEN TO:
- Newborns in incubators who are resting on lines or tubes.
- People with spinal cord injuries who have lost sensation and don’t feel uncomfortable sitting in the same position day after day—and therefore don’t realize that their skin is being affected.
- People who are bed bound and who are unable to change their position in bed.
Although pressure ulcers can develop anywhere on the body, they are more likely to occur on the buttocks of people who sit in a chair all day or in the heels, above the tailbone, and on the insides of the elbows of people who have to stay in bed all day.
Pressure ulcers can result from friction injuries to the skin when a person is being pulled across a surface, such as being pulled across a sheet when the bed is being made or being pulled out of a wheelchair.
SKIN ALSO CAN BE INJURED BY PROLONGED EXPOSURE TO TAPE, URINE, AND FECES, OR IT MIGHT BE INJURED BY TAPE REMOVAL. ALTHOUGH THESE INJURIES MIGHT LOOK SIMILAR TO A PRESSURE ULCER, THEY OFTEN AREN’T. HOWEVER, THIS KIND OF WOUND IS MORE LIKELY TO BECOME A PRESSURE ULCER IF THE SKIN IS EXPOSED TO TOO MUCH OR TOO LITTLE MOISTURE, SCRUBBING, OR TEMPERATURES THAT ARE TOO COOL OR TOO WARM.
SIGNS AND SYMPTOMS
Many people with pressure ulcers don’t know that they have one. Pressure ulcers might first be seen by a family member, a caregiver, or a physical therapist or other health care provider.
Pressure ulcers might be noticed when bathing or dressing someone who is at risk for developing them. A foul odor or the presence of yellow, brown, or gray mushy material on bedding or clothing might be noticed first and traced to an opening in the skin. Although pressure ulcers can be very painful, the person who has the ulcer might not notice any pain or might have pain but not be able to communicate it.
How Is It Diagnosed?
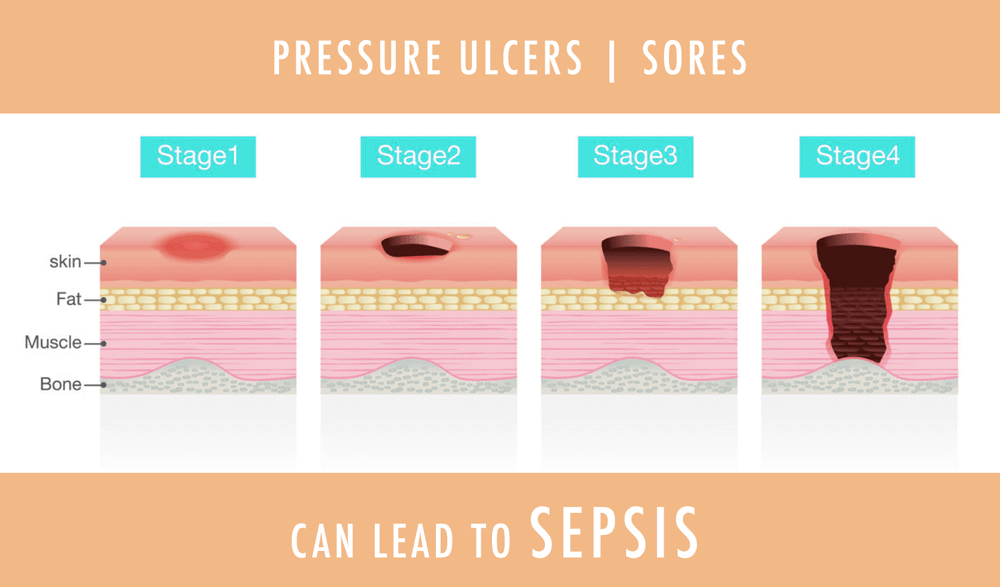
THE PHYSICAL THERAPIST WILL CONDUCT A FULL EVALUATION, INCLUDING STAGING THE PRESSURE ULCER BASED ON A SYSTEM DEVELOPED BY THE NATIONAL PRESSURE ULCER ADVISORY PANEL (NPUAP):
- Stage I ulcer – persistent reddening of the skin due to staying in the same position for too long. In darker skin, the skin might look purple. The skin might feel warmer to the touch than the surrounding skin.
- Stage II ulcer – shallow wound that goes only partially into the skin, usually caused by friction.
- Stage III ulcer – a deeper wound that goes through all of the layers of the skin, including fatty tissue under the skin.
- Stage IV ulcer – a wound that goes deeper than just the skin, down into the muscle, tendon, ligament, or bone; it might even expose nerves and blood vessels.
These stages don’t necessarily tell how severe a pressure ulcer is, and ulcers don’t always progress from one stage to the next. What looks like a “simple” stage I ulcer might be a minor irritation of the skin—or might be hiding a large mass of injured tissue beneath.
If there are blood-filled blisters, or purple or maroon areas of what appears to be uninjured skin, that could mean the tissue beneath the uninjured-looking skin is dead. On the other hand, there might be extensive death of tissue such as muscle, but the skin might not look injured at all. This is why a large ulcer might seem to appear “out of nowhere” within a matter of a few days. Muscle and other tissue near bone may be damaged by pressure before the skin breaks down, revealing a large wound extending to the bone. Detailed examination by a physical therapist or other health care provider is needed.
BASED ON THE EXAMINATION, THE PHYSICAL THERAPIST WILL DECIDE WHETHER ANY FURTHER TESTING OR CONSULTATION WITH ANOTHER HEALTH CARE PROVIDER IS NECESSARY. IN SOME CASES, SURGERY OR THE PRESCRIPTION OF ANTIBIOTICS BY A PHYSICIAN MAY BE NECESSARY.
How Can a Physical Therapist Help?
Physical therapists are skilled in wound care. Based on the results of the physical therapist’s evaluation, including a review of the medical history and an examination of the wound, the therapist will select treatments, which may include caregiver training, strengthening exercises, wound care, improvements to the seat or bed, and coordination with other health care providers.
TRAIN THE FAMILY AND CAREGIVERS IN REPOSITIONING
Because pressure ulcers are usually the result of prolonged contact of a body part with a bed or chair, repositioning or moving a person back and forth between a bed and a chair is needed to help pressure ulcers heal. Physical therapists are experts in positioning people on different surfaces, including beds, wheelchairs, toilets, bedside commodes, or other types of chairs and furniture as well as in moving a person from one surface to another (called “making transfers”). The physical therapist can train family members and caregivers to do positioning and transfers safely.
IMPROVE STRENGTH
In many cases, pressure ulcers are the result of people being too weak to change their own position. The physical therapist will develop an exercise program so that the individual with pressure ulcers can help perform repositioning and transfers, in turn helping to prevent injury to caregivers. In some cases, a person with a pressure ulcer may regain the ability to do repositioning without any help.
CARE FOR WOUNDS
The physical therapist is trained in wound care and knows how to remove “nonviable,” dead tissue from a wound (“debridement”). The therapist may use sharp instruments such as scissors, scalpels, or curettes. Extensive debridement that requires cutting of surrounding healthy tissue or that requires general anesthesia would be performed by a surgeon.
Pressure ulcers require appropriate dressings to aid healing. Dressings include a suitable material to cover wounds and to fill deeper wounds. The physical therapist determines the type of dressing to use and how frequently it must be changed. In most cases, caregivers can be trained by the physical therapist to clean wounds and to change dressings. As a pressure ulcer heals, the ulcer likely will change, and so will the treatment. The physical therapist will evaluate the wound with each visit and determine the type of dressing to use and how often it should be changed.
The physical therapist will discuss what to expect in terms of normal wound healing, signs to look for that might indicate a problem between visits, and when to contact a physician or an emergency department.
IMPROVE SITTING AND LYING SURFACES
The surface on which a person lies or sits may contribute to pressure ulcers. The physical therapist will examine the types of surfaces being used and, if necessary, will make recommendations for a different surface. Recommended support surfaces may include specialized beds, mattresses, or cushions made of materials that decrease the amount of pressure on vulnerable parts of the body.
COMMUNICATE WITH OTHER HEALTH CARE PROVIDERS
A number of health care providers may be involved in the care of a person with a pressure ulcer. A physical therapist will communicate and coordinate care with physicians, nurses, dietitians, and others to ensure as much as healing as possible and to prevent new ulcers.
Can This Injury or Condition Be Prevented?
If no changes are made to the care of a person who has developed a pressure ulcer, another pressure ulcer is likely to develop in the same or a different place on the body. To help reduce the risk of a new ulcer, the physical therapist trains caregivers in positioning, transferring, and selecting support surfaces. But the best way to prevent a new pressure ulcer is to increase the ability to move. Although independent mobility is not always possible, many people with a pressure ulcer can learn to reposition themselves in bed or in a chair to reduce the risk.
REAL LIFE EXPERIENCES
Ellen T., an 80-year-old woman with congestive heart failure, chronic obstructive pulmonary disease, and Alzheimer disease, lives with her children and grandchildren. She is not capable of changing her own position in bed or in a chair, and her ability to communicate is limited. She has a private attendant on weekdays, and a physical therapist is scheduled to begin home health visits to improve her mobility.
One day while her daughter-in-law Megan is bathing her, Megan notices thick, mushy material on the sheet and a bad smell. Based on the location of the material on the sheet, Megan traces it back to Ellen’s tailbone, where there is an opening in the skin the size of a dime. She also notices that Ellen has shallow ulcerations on the back of both heels and the inner surfaces of both elbows. What does she do next?
Pressure ulcers can be very serious and can become infected. They require immediate attention. When Ellen’s physical therapist arrives that afternoon, the therapist examines the wound and recommends that Ellen be brought to her primary care physician to determine whether antibiotics are needed. Fortunately, no infection is found.
The therapist teaches the family how to clean and dress the wound and evaluates Ellen’s potential for greater mobility, showing the family how to reposition and transfer her from one surface to another. The therapist will continue to work with this family until the wound is clean and stable enough for the family to manage the pressure ulcer at home and Mrs T has as much mobility as possible.
This story was based on a real-life case. Your case may be different. Your physical therapist will tailor a treatment program to your specific case.
During your first visit with the Therapy West’s physical therapists, be prepared to describe your symptoms in as much detail as possible, and say what makes your symptoms worse.